Pharmacy First has been described as a pivotal shift for community pharmacy. It signals trust in pharmacists as frontline clinicians, expands access for patients, and aims to relieve pressure on general practice. On the surface, it appears to be an elegant solution: care delivered closer to home, funded at a fixed rate, embedded within existing pharmacy settings.
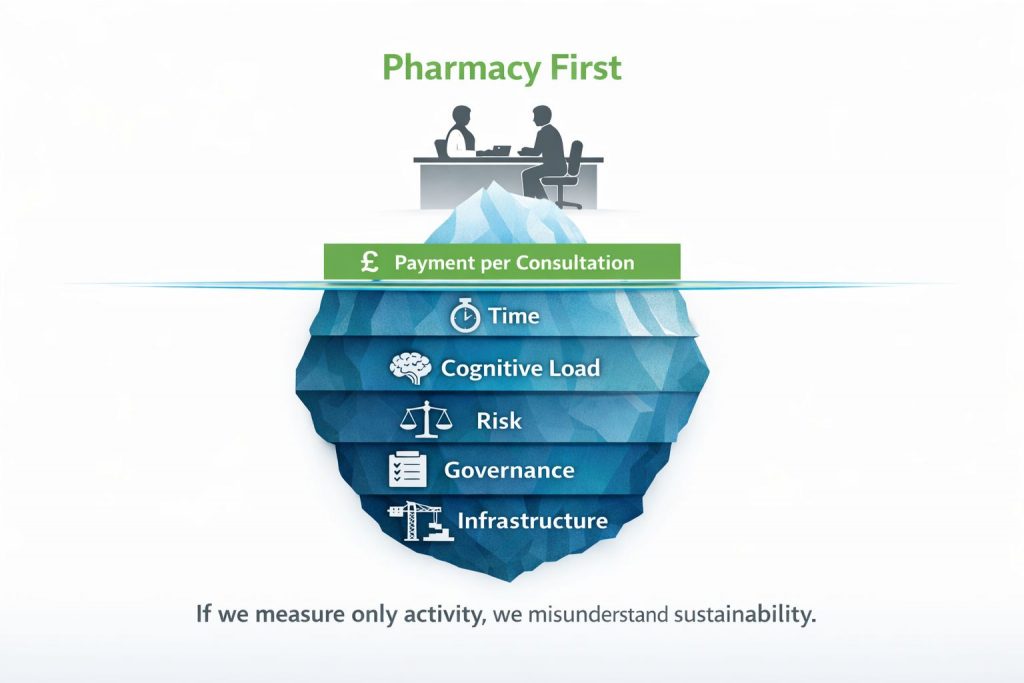
Yet the true cost of Pharmacy First is more complex than reimbursement figures suggest. The visible financial payment per consultation tells only part of the story. Beneath it sits a deeper operational reality shaped by time, cognitive demand, governance responsibility, and system infrastructure. If we are serious about sustainability, these dimensions must be examined with the same attention as activity numbers.
The first cost is time, and it is consistently underestimated. A Pharmacy First consultation may be labelled as brief, but in practice it rarely exists in isolation. It is delivered within a live dispensing environment, interrupted by workflow pressures, queries from staff, and competing patient demands. The consultation itself requires structured history taking, red flag identification, clinical reasoning, documentation, safety-netting advice, and submission of claims. What might appear to be a ten-minute interaction often becomes twenty minutes of end-to-end clinical engagement. When multiplied across daily volumes, this incremental extension becomes significant. It does not simply absorb minutes; it absorbs capacity. Capacity that was previously allocated to dispensing, supervision, prescribing support, or managerial oversight is quietly redistributed.
Beyond time lies a more subtle cost: cognitive load. Pharmacy First elevates the clinical responsibility of pharmacists. With that elevation comes a shift in professional risk. Each consultation requires judgement under time pressure. Each red flag must be recognised. Each documentation entry must withstand audit scrutiny. The mental bandwidth required to maintain vigilance across repeated consultations in a high-throughput environment should not be underestimated. Cognitive fatigue is not visible on a balance sheet, yet it directly influences safety, consistency, and resilience. When a service expands rapidly without corresponding structural support, variability can increase. And variability, in clinical settings, is rarely neutral.
Risk is therefore not an abstract concern but a measurable dimension of cost. As community pharmacies assume greater frontline responsibility, their exposure to complaints, audit queries, and regulatory scrutiny naturally increases. Documentation standards must remain robust. Referral decisions must be defensible. Clinical reasoning must be reproducible. In a model that depends heavily on individual practitioner judgement, the absence of structured infrastructure can amplify variability between sites. Over time, such variability can undermine confidence in the service, regardless of initial success metrics.
At the same time, it would be short-sighted to frame Pharmacy First solely in terms of burden. Its value proposition is substantial. It offers earlier access to treatment, reduces unnecessary GP appointments, and reinforces the role of pharmacy within integrated care systems. For many patients, it delivers timely reassurance and intervention that might otherwise have been delayed. These benefits carry system-level economic implications that extend far beyond the pharmacy counter.
However, true value cannot be assessed purely through activity volumes or reimbursement totals. It must account for sustainability. If consultation time consistently erodes workforce capacity, if cognitive load increases burnout risk, or if governance pressures escalate without structured mitigation, then short-term gains may compromise long-term stability. Measuring value without measuring cost creates an incomplete narrative.
This is where infrastructure becomes decisive. Structured consultation pathways, intelligent documentation support, and embedded clinical guidance can influence time, risk, and value simultaneously. By standardising elements of assessment while preserving professional judgement, infrastructure reduces unnecessary variability. By streamlining documentation, it reclaims time. By creating audit-ready records, it strengthens governance. In doing so, it transforms Pharmacy First from an additional responsibility layered onto existing workload into a systematised service capable of scale.
The conversation about Pharmacy First must therefore mature. Success cannot be judged solely by the number of consultations delivered. It must also be judged by how intelligently those consultations are supported. Time should be measured end-to-end rather than assumed. Risk should be quantified rather than overlooked. Value should be assessed in terms of resilience as well as revenue.
Pharmacy First represents a structural shift in the role of community pharmacy. Structural shifts demand structural support. If we measure only what is visible, we risk misunderstanding what is sustainable. If we measure time, risk, and value together, we create the foundation for a model that strengthens pharmacy rather than stretching it.
The future of Pharmacy First will not depend simply on expansion. It will depend on whether the systems surrounding it evolve with equal ambition.