| PHARMBOTAI | THOUGHT LEADERSHIP The promise of AI in pharmacy is real — but so is the gap between capability and clinical usability. Here is what we have learned building AI infrastructure for the frontline of NHS pharmacy. Asif Mukhtar | Founder & CEO, Consultant Pharmacist | April 2026 |
| AI is not coming to healthcare. It is already here. The question facing every pharmacist, every ICB medicines optimisation lead, and every NHS system leader is no longer whether to engage with AI — it is whether to engage with the right AI, built in the right way, for the right reasons. |
These are insights drawn from our work building PharmBot AI — and from a recent webinar delivered to pharmacy professionals across Africa, where the questions being asked about AI in clinical practice were strikingly similar to those being asked here in the UK.
The Reality of AI in Pharmacy Today
The pharmacy sector is at a genuine inflection point. Through initiatives like Pharmacy First, community pharmacists are now delivering clinical consultations at scale — triage, prescribing decision support, medicines optimisation — across a primary care system under sustained pressure.
At the same time, AI tools are proliferating faster than the governance frameworks that should surround them. The result is a landscape full of impressive demonstrations and poor real-world adoption. Generic chatbots are being dressed up as clinical decision support. Tools built outside clinical workflows are being bolted onto them. And pharmacists — who remain legally and professionally accountable for every decision they make — are being asked to trust systems they cannot interrogate.
| Most AI conversations in healthcare are happening outside workflows. That is why they fail — not because the technology is bad, but because the conversation is happening in the wrong place. |
At PharmBot AI, we have been building inside the workflow from day one. Not theorising about what AI could do for pharmacy. Building it, testing it, learning from it, and rebuilding it — in real clinical environments, with real pharmacists, under real accountability pressures.
The Problem Is Not the Technology
The most important insight we have developed — and the one that underpins everything we build — is this: the failure of AI in healthcare is not a technology problem. It is an integration problem.
Most AI tools in healthcare fail for one of three reasons. They do not fit existing workflows, requiring clinicians to change how they work to accommodate the technology rather than the other way around. They offer no accountability — when an AI produces a recommendation, who is responsible for it? In healthcare, that ambiguity is not uncomfortable. It is dangerous. And governance is treated as an afterthought, bolted on after the product is built rather than designed in from the outset.
The pharmacist remains accountable — always. Any AI system that obscures that accountability, rather than strengthening it, has no place in clinical practice.
Capability Is Not the Same as Usability
A model can pass a pharmacy examination. It can answer drug interaction queries with impressive accuracy. But if a pharmacist cannot explain that answer to a patient, a GP, or the GPhC — they will not use it. And they should not.
This is the gap that most AI products fail to cross. Capability and usability are not the same thing. Building for capability is a technology challenge. Building for usability in a clinical environment is a human challenge — one that requires deep understanding of how pharmacists actually work, what they are accountable for, and what it means to be the last line of defence for a patient’s safety.
| Capability: | What the AI can technically do — accuracy, speed, breadth of knowledge. Necessary but not sufficient. |
| Usability: | Whether a pharmacist can use it, defend it, and trust it in a real clinical environment under real time pressure. |
| Governance: | Whether it meets GPhC standards, creates defensible audit trails, and keeps the pharmacist in control. |
| Integration: | Whether it fits seamlessly into existing workflows without adding cognitive load or extra steps. |
All four must be present. A tool with three out of four will not be adopted. In healthcare, partial solutions are not solutions — they are risks.
From Tools to Clinical Infrastructure
The most significant conceptual shift in how we think about AI at PharmBot AI is the move from tools to infrastructure. A tool is something you pick up and put down. It lives outside your workflow. It is optional. Most AI in healthcare is being built as tools — and that is why adoption rates remain low despite significant investment.
Infrastructure is different. Infrastructure is what you work through, not what you work with. It is the underlying layer that makes every clinical interaction faster, safer, and better documented — invisibly, reliably, consistently.
| We are not replacing pharmacists. We are structuring their thinking.PharmBot AI’s founding principle — the pharmacist remains in control, accountable, and central to every clinical decision. |
When AI is infrastructure, it does not add to the cognitive load of a busy pharmacist. It reduces it. The clinical knowledge does not change. The accountability does not change. But the environment in which clinical decisions are made is transformed — from reactive and fragmented to structured, consistent, and defensible.
What AIVAe Does in Practice
AIVAe is PharmBot AI’s AI-enabled virtual pharmacist — built specifically for NHS pharmacy workflows. Not adapted from a general-purpose large language model. Built from the ground up with pharmacists, for pharmacists, aligned with GPhC standards and NHS clinical pathways.
| Structured Consultations: | Guides Pharmacy First assessments through consistent clinical pathways, ensuring nothing is missed under time pressure. |
| SOAP Note Generation: | Auto-drafts GPhC-compliant consultation notes in seconds, freeing pharmacist time for patient care. |
| PGD-Aligned Reasoning: | Supports safe prescribing decisions with structured reasoning and a clear, auditable clinical trail. |
What AIVAe does not do is equally important. It does not replace pharmacists. It does not make final clinical decisions. It does not take accountability away from the registered professional. The pharmacist reviews every output, approves every recommendation, and retains complete clinical responsibility.
The Future Role of the Pharmacist
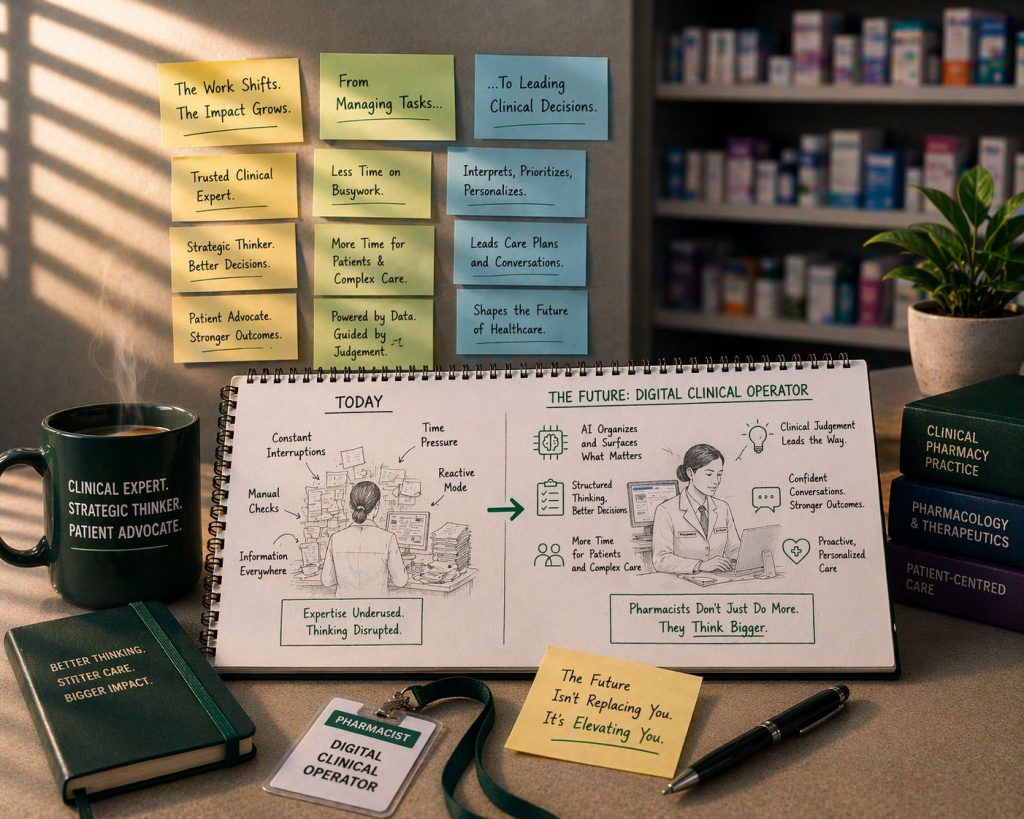
The pharmacist of the near future is not a passive user of AI tools. They are what we call a Digital Clinical Operator — someone who works through AI infrastructure to deliver faster, safer, more consistent care, while retaining the clinical judgement and human connection that no technology can replicate.
This is not a diminished role. It is an elevated one. Less time spent on documentation and routine checks means more time for complex clinical decisions, patient conversations, and the kind of professional leadership that the expanding scope of pharmacy demands.
The skills that matter most in this future are not technical. They are clinical reasoning — the ability to evaluate AI output, interrogate recommendations, and apply professional judgement. Structured thinking. Understanding of workflows. These are pharmacy skills, not technology skills. The pharmacist who develops them will be more valuable, not less, in an AI-enabled healthcare system.
What Good AI Adoption Looks Like
For pharmacy organisations, ICBs, and NHS system leaders thinking about AI adoption, we offer four practical principles drawn from our experience building in real clinical environments.
- Start with the workflow, not the tool. The question is not ‘what AI is available?’ — it is ‘where does our clinical workflow break down, and what would make it flow better?’ Tools that do not fit workflows will not be used, regardless of their technical capability.
- Governance cannot be retrofitted. Any AI system deployed in clinical pharmacy must be compliant with GPhC standards, GDPR, and NHS governance requirements from day one. If governance is an afterthought, the system is not deployable — and should not be deployed.
- Simplicity beats complexity. Every feature added to an AI tool should reduce the pharmacist’s cognitive load, not increase it. If a feature adds steps, adds uncertainty, or adds time — it does not belong in a clinical product.
- The pharmacist must remain accountable. AI in pharmacy must make pharmacists more defensible, more consistent, and more confident — not less. Any system that obscures clinical accountability is a liability, not an asset.
A Final Thought
AI will not transform pharmacy through novelty. It will transform pharmacy through integration — deep, thoughtful, governance-ready integration into the clinical environments where pharmacists do their most important work.
The technology is ready. The clinical case is clear. The NHS need is urgent. What has been missing is AI built by people who understand pharmacy from the inside — who know what it means to stand at the dispensary counter with forty patients waiting, a complex consultation to document, and a professional accountability that never shifts.
That is the problem PharmBot AI was built to solve. And it is only the beginning.
| Interested in learning more?PharmBot AI is working with NHS pharmacy networks and ICB partners across the UK.www.pharmbotai.com | info@pharmbotai.com |